
Biological aging among older Americans
The Growing Cost of Less Education: Biological Aging Among Older Americans
Mateo P. Farina, Jung Ki Kim, and Eileen M. Crimmins
Education has long been linked to better health. People with higher levels of education tend to live longer, have better physical and mental health, and report higher quality of life. These advantages come from a range of factors including better jobs and income, healthier environments, stronger social networks, better access to information and technology, and greater ability to navigate the healthcare system. On the other hand, people in more disadvantaged social positions, who are often those with less education, tend to experience more long-term stress, have higher rates of smoking, and are in more physically demanding jobs. These experiences can accumulate to produce more “wear and tear” on the body, leading to accelerated aging that puts people at greater risk of health complications.
Different levels of wear and tear can lead to different levels of biological aging, or how fast (or slowly) bodies age on the inside. In other words, biological aging is not how old someone is chronologically but rather how fast their bodies have aged due to stress, lifestyle, and other factors. For example, someone aged 50 who looks similar to someone aged 60 biologically is said to have accelerated biological aging. People with faster biological aging are at higher risk for serious health problems as they get older. And studies show that people with less education tend to age biologically faster.
The meaning and value of education have also changed over time. For much of the 20th century, a high school diploma could lead to a stable, well-paying job. But starting in the late 20th century, this pathway eroded. The loss of good blue-collar jobs, declining wages, and rising educational requirements for stable employment meant that people without a college degree began to fall further behind—not just economically but also in terms of health with greater risk of mortality and other health conditions like diabetes. This has happened at the same time that college educated adults are living more years and in better health. This has led to growing health inequality in the United States.
Biological aging is an important precursor to poor health in older ages. Understanding whether biological aging has followed similar patterns of inequality can help explain these trends and suggest new ways to intervene to reduce health inequalities.
This brief summarizes a recent study [1] in which the researchers used national health data to analyze how accelerated biological aging has changed for Americans aged 50 to 79 from the 1988 to 2018 across education levels. They also looked at whether changes in smoking, obesity, and use of medications (for things like high blood pressure or cholesterol) explained some of these differences.
By analyzing changes in biological aging across educational groups over time — and considering key behavioral and medical factors — this study sheds light on how educational inequality becomes embodied in the aging process. The findings aim to help researchers and policymakers better understand the root causes of growing health disparities and explore potential strategies to reduce them. Biological aging, as a marker of accumulated life stress and exposure, may be a powerful tool for identifying where and how interventions can make the most difference to improve health for older Americans.
KEY FINDINGS
-
Biological aging slowed for everyone across all education levels over the 25-year period between surveys. See figure
-
However, inequalities in biological aging increased between education groups because people with higher education experienced greater improvements. See figure
-
Growing inequality in biological aging was not explained by changes over time in smoking habits, obesity rates, or medication use.
Changes in biological aging over time by level of education: Findings
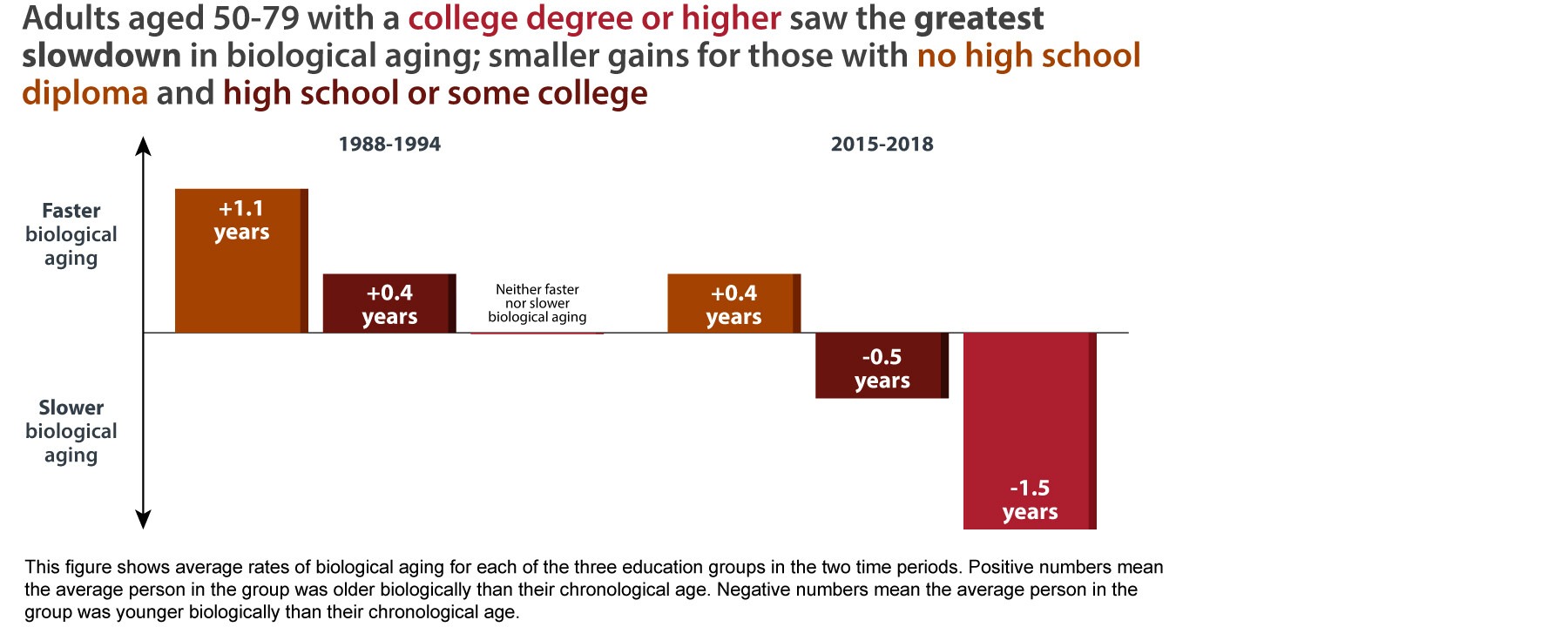
Between the late 1980s and late 2010s, biological aging slowed for older Americans across all education levels. However, the improvements were greatest for those with the most education, leading to a widening gap in how different education groups experience aging.
Biological aging slowed for everyone across all education groups (less than a high school diploma, a high school diploma or some college, and a college degree or higher). Biological aging more than halved for older Americans without a high school diploma who went from aging 1.1 years faster biologically in the 1988-1994 period to less than half a year (0.4) in 2015-2018; see figure. Older Americans with a high school diploma or some college also improved, going from aging faster by 0.4 years in the late 1980s/early 1990s to aging a half year slower in the more recent period. Older Americans with a college degree or higher saw the most improvements: they went from neither aging faster nor slower in 1988-1994 to aging 1.5 years more slowly in 2015-2018.
Because of the larger gains for older American with the highest levels of education, educational inequality increased across time. The difference in biological aging between the highest and lowest educated grew from a one-year difference in 1988-1994 to almost two years in 2015-2018; see figure.
By examining how health behaviors and medication use were associated with aging within each education group, the authors found that obesity was strongly linked to faster aging in every group, while smoking showed no significant effect. Taking blood pressure medication was associated with accelerated aging in all groups; taking cholesterol medication was also linked to faster aging, but only for the most educated group. Although biological aging slowed overall, rising obesity and increased medication use—likely reflecting underlying health issues—reduced even greater potential gains. Without these health challenges, all education groups would have experienced even greater improvements in biological aging.
Policy Implications
Biological aging has slowed in the U.S., but gains are concentrated among highly educated adults, leaving those with lower education levels at greater risk of poorer health in later life. To close this gap, policies should expand access to healthy environments, preventive care, and aging-related resources for less educated populations. At the same time, public health efforts must address modifiable risk factors for all people—particularly obesity, poor diet, physical inactivity, and unmanaged chronic conditions—while ensuring equitable access to emerging obesity treatments such as GLP-1 medications. Finally, integrating measures of biological aging into public health surveillance can serve as an early warning system, enabling earlier identification of at-risk groups and more timely, targeted interventions to reduce health disparities.
Data and Methods
The researchers used data from the National Health and Nutrition Examination Survey (NHANES) from 1988-1994 and 2015-2018. NHANES is a nationally representative survey of the non-institutionalized U.S. population. The researchers analyzed data from 9701 adults ages 50 to 79 (5415 from 1988-1994 and 4286 from 2015-2018). To measure biological aging, the researchers used eight biomarkers that are related to aging and health outcomes: Hemoglobin A1c, total cholesterol, serum creatinine, systolic blood pressure, alkaline-phosphate, albumin, C-reative protein, and Blood Urea Nitrogen. They created three education categories based on the number of years of schooling: 0 to 11 years of education (no high school diploma), 12-15 years of education (completed high school but did not obtain a bachelor’s degree), and 16 or more years of education (obtained at least a bachelor’s degree).
To analyze the data, the researchers first calculated change in biological age acceleration for each education group between 1988-1994 and 2015-2018. Next, they examined how health behaviors and medication use changed from 1988-1994 to 2015-2018 for each education group to understand how these population health risk factors changed over time. Then they estimated a series of linear regression equations to evaluate how differences in biological aging between education groups changed over time and whether those differences were affected by including smoking, obesity, and medication use.
Reference
[1] Farina, M.P., Kim, J.K., & Crimmins, E.M. (2025). Increasing educational inequality in biological aging among adults 50-79 in the United States from 1988-1994 to 2015-2018. Demography 12175545. https://doi.org/10.1215/00703370-12175545
Suggested Citation
Farina, M.P., Kim, J.K., & Crimmins, E.M. (2025). The growing cost of less education: Biological aging among older Americans. CAPS Research Brief 4(2). https://doi.org/10.26153/tsw/61180
About the Authors
Mateo Farina, mateo.farina@austin.utexas.edu, is an assistant professor in the Human Development and Family Sciences Department, a faculty affiliate in the Center for Aging and Population Sciences and a faculty scholar in the Population Research Center at The University of Texas at Austin; Jung Ki Kim is a research associate professor of gerontology in the University of Southern California Leonard Davis School of Gerontology; and Eileen M. Crimmins is a University Professor and the AARP Chair in Gerontology at the USC Leonard Davis School of Gerontology.
Acknowledgements
This research was supported by the National Institute on Aging (grant numbers P30 AG043073, T32 AG000037, P30 AG17265, R01 AG060110, K99AG076964; R00AG076964). The research brief was supported by grant P30AG066614, awarded to the Center on Aging and Population Sciences at The University of Texas at Austin by the National Institute on Aging. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.