
Black-White mental health paradox across U.S. regions
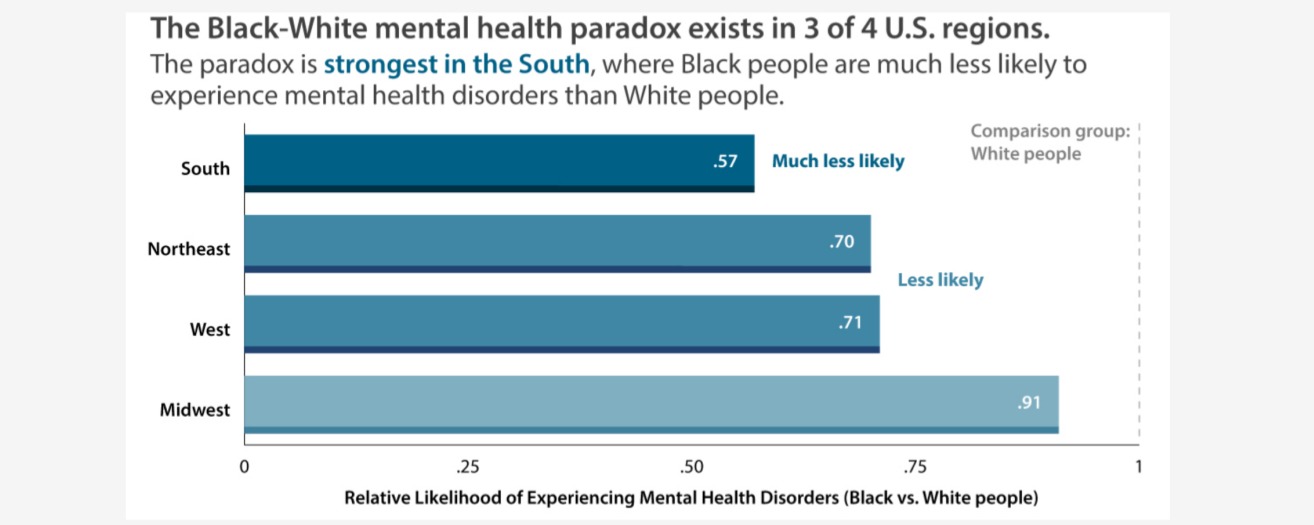
Black-White Mental Health Paradox is Strongest in the South, Compared to Other Regions in the U.S.
Christy L. Erving, Lacee A. Satcher, Shania Montúfar, Courtney S. Thomas Tobin
In the United States, the “Black-White mental health paradox” describes a pattern in which Black people have similar, and often lower, rates of psychiatric disorders than White people. This pattern contradicts the expectation, based on social stress theory, that historically disadvantaged people facing greater exposure to social stress would have higher rates of mental disorder.
Not much is known about how the pattern differs by region. Understanding how patterns of mental disorders differ by race within regions is crucial for several reasons. First, research could show that the pattern exists across all regions in similar or different ways. Second, research could identify regions, racial groups, and mental health disorders where prevention and intervention efforts should be targeted. Third, looking at patterns of mental disorder by race within regions can shed light on how structural racism and its effects differ by region.
Many studies demonstrate that the prevalence of physical health problems varies across regions. Some evidence suggests the prevalence of any mental disorder in the past year may similarly vary across regions. Evidence also suggests that psychological well-being and specific mental disorders vary among Black and White Americans across regions. However, these studies typically examine mental health only for one racial group and do not compare racial groups.
This brief is based on a recent study [1] that fills a research gap by comparing rates of psychiatric disorders among Black and White people across four U.S. geographical regions and exploring whether patterns differ by type of mental disorder. Using data from the National Comorbidity Survey-Replication and the National Survey of American Life, the authors assessed the three most common categories of psychiatric disorder and their diagnoses in the past year: any mood disorder (major depressive disorder, bipolar 1 and 2, dysthymia), any anxiety disorder (panic disorder, agoraphobia, social phobia, generalized anxiety disorder, post-traumatic stress disorder), and any substance use disorder (alcohol abuse, alcohol dependence, drug abuse, drug dependence). The authors also assessed any mental disorder, which includes any mood disorder, any anxiety disorder, and substance disorder. Their study answers the question, does the Black-White mental health paradox exist across U.S. regions in the same way?
Key Findings
-
The Black-White mental health paradox was found in three of four U.S. regions, even after accounting for differences in sociodemographic factors between Black and White people living in those regions.
-
The Black-White mental health paradox was strongest in the South, where Black people were less likely to experience mood, anxiety, and any mental health disorders than White people.
-
The mental health paradox was also found in the Northeast and West, but it was not as strong. In those regions, Black people were less likely to experience any mental health disorder than White people.
-
In the Midwest, however, evidence for the paradox was weak. In that region, Black people were more likely to experience a mood disorder compared to White people. The higher rate of mood disorders among Black people in the Midwest was partially due to Black Midwesterners’ lower educational attainment and employment rates compared to White Midwesterners.
The Black-White mental health paradox was the strongest in the South. Black people living in the South were less likely to experience psychiatric disorders compared to White people in the South, even after accounting for sociodemographic factors. In the South, Black people seemed to have better mental health than White people even in the face of their lower educational attainment, lower rates of marriage or cohabiting, and younger ages, compared to White people (see figure).
In the Northeast and West, the paradox existed for any mental disorder in the past year. In both regions, Black people were less likely to experience any mental disorder in the past year compared to White people even after accounting for socioeconomic factors. That means that in the Northeast and West regions, Black people would show even better overall mental health than White people if Black people did not have lower levels of education and marriage or cohabitation than White people (see figure).
In the Midwest, however, evidence for the paradox was weak. In this region, Black people were more likely to experience mood disorders compared to White people. Much of this difference can be explained by Black people’s lower employment status and educational attainment. In the Midwest, there were no racial differences in anxiety disorder, substance use disorder, or any mental disorder in the past year after accounting for socioeconomic factors.
Policy Implications
Mental health intervention and prevention programs should be tailored to specific U.S. regions. The advantage that Black people have for mental health in the South, even with Black people’s socioeconomic disadvantage, highlights the importance of fighting structural racism and exploring protective factors such as a critical mass of Black residents, strong ethnic identity, and strategies people use to stay healthy that may be specific to the South. This recommendation is bolstered by several studies that show structural racism, as measured across educational, judicial, economic, political, and segregation domains, is highest in the Midwest and Northeast and lowest in the South.
Higher rates of mood disorders among Black people compared to White people in the Midwest show the need for targeted interventions in this region. This study suggests that efforts to address racial inequalities in access to education, employment, and other economic resources in the Midwest may help to decrease the rate of mood disorders among Black people.
Data and Methods
Sample. The researchers merged the National Comorbidity Survey-Replication and the National Survey of American Life to create a large, nationally representative sample of U.S.-born non-Hispanic African Americans and White Americans. The sample included 4,584 Black people and 6,668 White people (total N=11,252).
Measures. To assess psychiatric disorders, the researchers used the World Mental Health Survey Initiative version of the World Health Organization Composite International Diagnostic Interview (WMH-CIDI). They included three measures of the most diagnosed categories of psychiatric disorder: any mood disorder, any anxiety disorder, and any substance use disorder. They also included risk for any mental disorder (a compilation of the three disorders). Key independent measures included race, which was self-reported by survey respondents, and current region of residence. The analyses also accounted for sociodemographic and other characteristics such as educational attainment, employment status, marital status, sex, and age.
Analysis. Due to the data’s complex sampling strategy, the study corrected for the sample’s unequal probabilities of selection, non-response, and design effects. The researchers applied 1) means and frequencies to examine measures described above by region and race, and 2) a series of binary logistic regression models to assess racial patterns for each disorder category within each region before and after accounting for sociodemographic factors.
Reference
[1] Erving, C.L, Satcher, L.A., Montúfar, S., & Thomas Tobin, C.S. (2025). Does the Black-White mental health paradox persist across U.S. geographical regions? SSM - Mental Health 7(100431).
https://doi.org/10.1016/j.ssmmh.2025.100431
Suggested Citation
Erving, C.L, Satcher, L.A., Montúfar, S., & Thomas Tobin, C.S. (2025). Black-White mental health paradox is strongest in South, compared to other regions in U.S. Population Research Center Research Brief 10(5). https://doi.org/10.26153/tsw/60738
.
About the Authors
Christy L. Erving, christy.erving@austin.utexas.edu, is an associate professor of sociology at The University of Texas at Austin and a faculty research associate in the Population Research Center; Lacee A. Satcher is an assistant professor in the department of Sociology and Environmental Studies at Boston College; Shania Montúfar is a PhD student in sociology and a PRC Graduate Research Trainee at UT Austin; and Courtney S. Thomas Tobin is an associate professor in the department of Community Health Sciences at UCLA’s Fielding School of Public Health.
Acknowledgements
This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (P2CHD042849), awarded to the Population Research Center at UT Austin and a Robert Wood Johnson Foundation Health Policy Research Scholars Award. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or other funders.