
Post-Migration Stressors Take a Toll on Refugee Health
Post-Migration Stressors Take a Toll on Refugee Health
Matthew Blanton, August 2025
Key Findings
-
Stressful experiences and events after migration led to mental distress and problems like anxiety and depression.
-
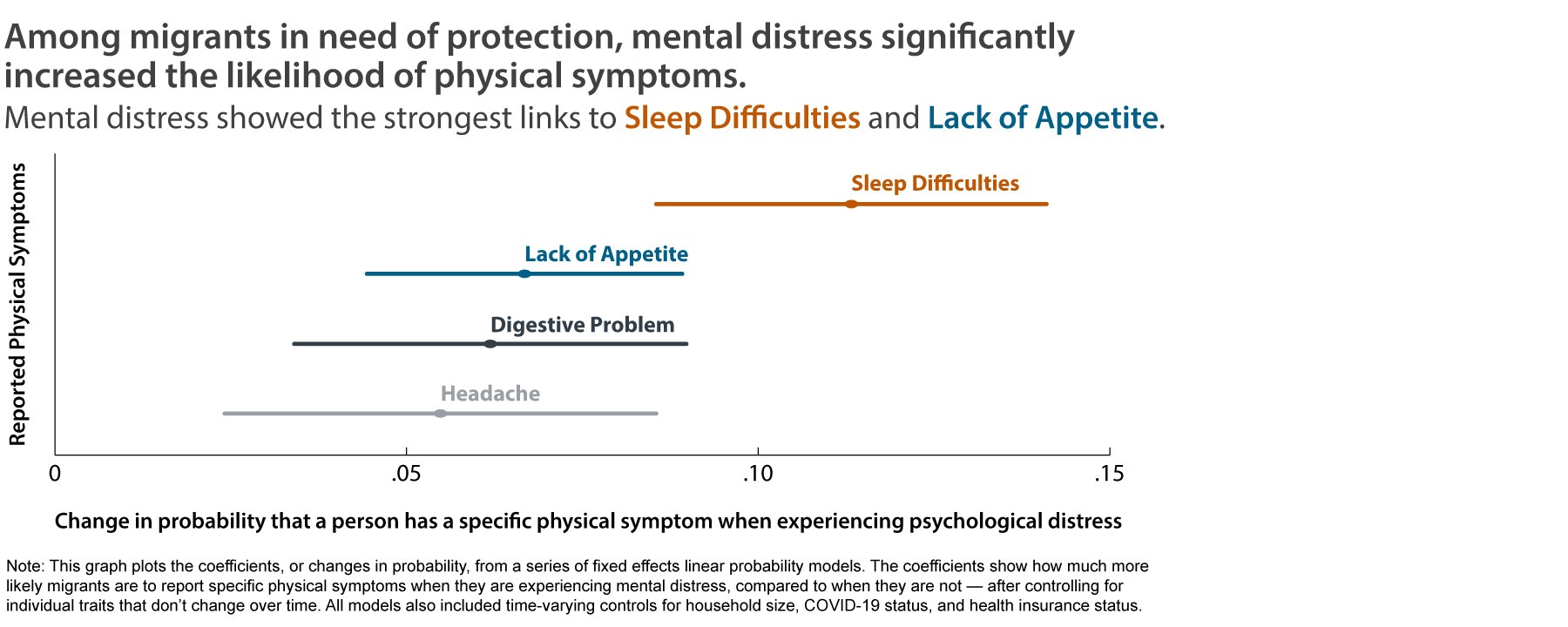
Among migrants in need of protection, mental distress (caused by stressors) led to problematic physical symptoms.
-
Physical symptoms usually went away quickly once stress levels dropped.
-
Economic hardship, discrimination, and ongoing separation from family members were the biggest factors affecting mental and physical health.
-
Migrants in need of protection clearly understood and described how stress affected their bodies.
Stressful experiences and events after migration led to mental distress and problems like anxiety and depression. When migrants to Costa Rica faced problems such as job loss, discrimination, or poor housing, their mental health suffered. These experiences led to increased feelings of sadness, anxiety, and loneliness.
Mental distress (caused by stressors) led to problematic physical symptoms. When people who migrated felt emotionally unwell, they often immediately experienced physical issues, including sleep difficulties, lack of appetite, digestive problems and headaches. Mental distress was most strongly linked to sleep difficulties (see figure). These physical symptoms come and go quickly, closely tied to weekly changes in stress levels.
Physical symptoms usually went away quickly once stress levels dropped. Physical symptoms fluctuated closely with mental distress and stressful experiences and events, suggesting the potential for rapid improvement through targeted interventions.
Economic hardship, discrimination, and ongoing separation from family members were the biggest factors affecting mental and physical health. High cost of living, unemployment, losing housing, or being separated from loved ones caused major stress and health problems. When these issues improved, physical symptoms often disappeared.
Migrants in need of protection understood and described how stress impacts their bodies. In interviews, many migrants explained how stressful events affected their emotions and led to physical problems. They showed clear awareness of these links. Migrants described how stressful experiences and events led to distress and then to physical symptoms, challenging assumptions that marginalized groups lack insight into their own health.
Policy Implications
Governments and service providers should not only focus on the trauma migrants experienced before migration. They must also address discrimination, poverty, housing instability, separation from family members, and other stressors among migrants in their new home countries. These stressful experiences and events cause mental distress and harmful physical symptoms among refugees, asylum seekers, and other migrants in need of protection.
Policies that make it easier for migrants to work or reunite with family decrease stress and improve health. Reforms that improve access to legal work and facilitate family reunification can quickly improve both mental and physical health for migrants in need of protection. Facilitating access to stable employment through streamlined recognition of foreign educational or professional credentials, helping employers comply with labor laws, and reducing bureaucratic barriers can directly reduce mental distress, improve physical well-being, and ultimately lead to reduced healthcare costs and stable employment. Targeted reforms can benefit both individuals and society.
Data and Methods
Design. This study used a mixed-methods design. The author collected qualitative and quantitative in multiple phases, and each stage of research informed the next. All research was done in Spanish.
Data sources and samples. For the quantitative data, the author used the Survey of Refugees: Social Experiences and Health survey (ERESS), which is a 13- week longitudinal survey of adult migrants who need protection in Costa Rica. Some 247 adults completed the survey October 2021 to April 2022. For the qualitative data, the author and his research team conducted 65 in-depth interviews with female adult migrants from Nicaragua, Venezuela, Cuba, and El Salvador who need protections who had lived in Costa Rica for at least six months. Interviews took place in early 2020 and then again in late 2022. For all data collection, the author and his research team collaborated with and recruited through Fundación Mujer, a private nonprofit in Costa Rica with over 25 years of experience serving migrants who need protection.
Measures. The survey asked about demographics, household structure, adverse childhood events, pre-migration violence exposure, migration history and status; socioeconomic incorporation, mental and physical health; and local and transnational family dynamics. Questions on mental health covered stress, sadness, difficulty concentrating, loneliness, life satisfaction, and level of nervousness. Questions on physical health covered physical symptoms linked to stress such as sleep difficulties, lack of appetite, digestive problems and headaches. The survey also included questions on causes of stress after migration and other variables thought to influence mental and physical health.
Analysis. For the quantitative data, Blanton used fixed effects Ordinary Least Squares, Poisson, and linear probability models to analyze the relationships among stressors, mental distress, and physical symptoms in Costa Rica. For interviews, the author and his research team coded and analyzed the transcripts in Spanish, identifying primary and emergent themes.
Reference
[1] Blanton, M. (2025). Post-migration stressors and mental and physical health among refugees and migrants in need of protection: a mixed-methods analysis with weekly panel data. Society and Mental Health, 0(0). https://doi.org/10.1177/21568693251345117
Suggested Citation
Blanton, M. (2025). Post-migration stressors take a toll on refugee health. Population Research Center Research Brief 10(09). https://doi.org/10.26153/tsw/61104
About the Author
Matthew Blanton, mblanton@utexas.edu, is a PhD candidate in sociology and a trainee at the Population Research Center at the University of Texas at Austin.
Acknowledgements
This work was supported by grant P2CHD042849 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) awarded to the Population Research Center at UT Austin; NICHD grant K01HD099313 (PI: Weitzman); and NICHD grant T32HD007081 (PI: Blanton). The content is solely the responsibility of the author and does not necessarily represent the official views of the National Institutes of Health.