
Cardiovascular disease among mothers aged 30 to 45
Inequities among Individuals, Neighborhoods, and Counties Affect the Likelihood of Cardiovascular Disease for Mothers during the “Rush Hour of Life”
Catherine Cubbin, Quynh Nhu (Natasha) B. La Frinere-Sandoval, and Elizabeth M. Widen
"Established adulthood” covers the years 30 to 45 and is marked by occupational, familial, and caregiving demands that can affect women’s health. Established adulthood is often considered the “rush hour of life,” especially for mothers, who typically shoulder more caregiving responsibilities than fathers. In the United States, it is likely that race and ethnicity, country of birth, and socioeconomic status influence the experience of established adulthood. Alarmingly, cardiovascular disease seems to be increasing among women during this rush hour of life. Black, Hispanic, immigrant, and lower-educated women are particularly vulnerable to the disease during this life stage.
Cardiovascular disease encompasses a range of conditions affecting the heart and blood vessels and is the leading cause of death among women in the U.S. In addition to race and ethnicity, country of birth, and socioeconomic status being associated with the disease itself, these characteristics also influence risk factors for the disease, including diabetes, hypertension, obesity, and smoking. The neighborhoods in which women live can also influence risk factors for cardiovascular disease. Women of color and those with lower socioeconomic status are more likely to live in neighborhoods characterized by poverty and limited access to resources that promote health and wellness. Compared to urban counties, rural counties have fewer employment, childcare, and healthcare opportunities. These disadvantages at the individual, neighborhood, and county levels contribute to higher rates of risk factors for cardiovascular disease.
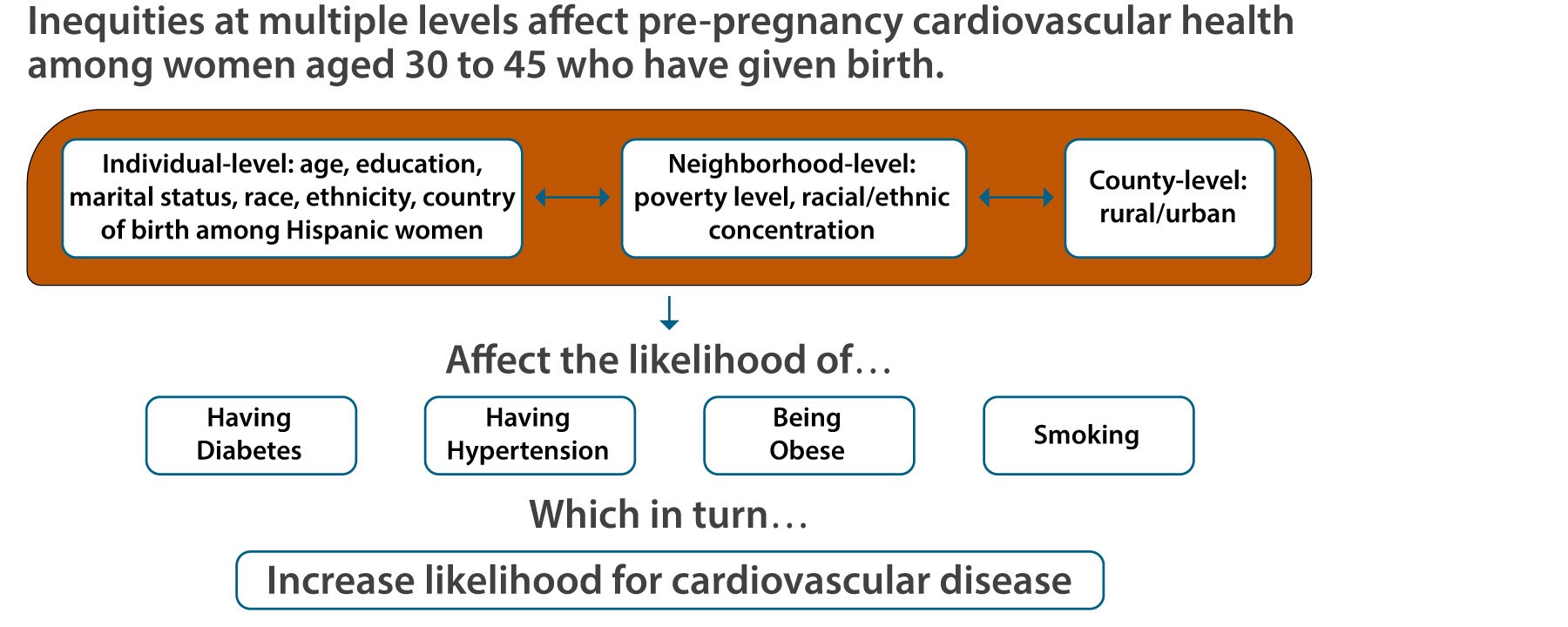
This brief is based on a study [1] that examined the prevalence of four pre-pregnancy risk factors (diabetes, hypertension, obesity, and smoking) for cardiovascular disease among women, aged 30 to 45, who gave birth. Using data from 2005 to 2020, the authors employ the ecosocial and life course theories to explore how individual, neighborhood, and county-level factors interact to produce disparities in experiencing the four risk factors. Ecosocial theory posits that structural and contextual factors work at multiple levels to influence health outcomes. Ecosocial theory and the life course perspective assume that risk accumulates over time and social factors “get into the body” and influence health outcomes during a specific life stage, like established adulthood. The authors draw on data at the individual, neighborhood, and county level from Texas, one of the most racially and geographically diverse states in the U.S. Findings from this study can inform policy and interventions to support women through this critical life stage.
Key Findings
-
Individual-, neighborhood-, and county-level factors work together to produce disparities in experiencing the four risk factors (diabetes, hypertension, obesity, and smoking) for cardiovascular disease.
-
Which characteristics increased the likelihood of women having the four risk factors for cardiovascular disease?
-
Lower levels of education
-
Living in neighborhoods with high poverty
-
Living in rural areas
-
Which characteristics mattered for women’s cardiovascular health?
-
Country of birth among Hispanic women
-
Race and ethnicity
-
Being married
-
Racial and ethnic makeup of neighborhoods
Factors at different levels interact to produce disparities in risks for cardiovascular disease. Among women aged 30 to 45 who have given birth, individual-, neighborhood-, and county-level factors worked together to produce disparities in experiencing diabetes, hypertension, obesity, and smoking.
Which characteristics increase the likelihood of women having the four risk factors for cardiovascular disease?
-
Lower levels of education increased the likelihood of having the four risk factors for cardiovascular disease. The likelihood of having diabetes went down with increasing education. College graduates were least likely to have any of the risk factors for CVD. Women without a high school degree were five times more likely than college graduates to smoke.
-
Living in neighborhoods with high poverty increased the likelihood of having the four risk factors for cardiovascular disease. Women living in neighborhoods with higher poverty were more likely to have diabetes, have hypertension, be obese, and smoke.
-
Living in rural areas increased the risk for cardiovascular disease. Women living in rural areas were more likely than other women to have diabetes, have hypertension, and be obese and much more likely to smoke (see figure).
Which characteristics mattered for women’s cardiovascular health?
-
Country of birth among Hispanic women, race, and ethnicity mattered for CVD health. Compared with White women, every other racial and ethnic group had a higher likelihood of having diabetes. This was especially of U.S.-born Hispanic women, who were twice as likely to have diabetes as White women. Black and U.S.-born Hispanic women were more likely than other women to have hypertension and be obese. White women were most likely to smoke.
-
Being married mattered for cardiovascular health. Women who were not married were more likely to have hypertension and be obese. They were three times more likely than married women to smoke.
-
The racial and ethnic makeup of neighborhoods mattered for cardiovascular health. Living in a neighborhood with a relatively high concentration of Hispanic people increased the likelihood for diabetes. Concentrations of Hispanic or Black populations were linked to a higher likelihood of having hypertension, being obese, and smoking. However, the likelihood of having these three risk factors plateaued or weakened as the concentrations of Hispanic and Black people within a neighborhood increased past a certain point.
Policy Implications
This study underscores the need for multi-level interventions to improve cardiovascular health to reduce disparities in cardiovascular disease among women aged 30 to 45. For example, interventions can target individual people, whole neighborhoods, and whole counties. Individual-level policies that improve the health of women and especially mothers during established adulthood are needed. Neighborhood-level policies must make whole neighborhoods healthier places to live. Policies aimed at decreasing poverty within a neighborhood, improving health infrastructure in rural areas, and investing in community development are essential. At the county level, county governments can encourage comprehensive plans for a county’s growth and prioritize a wide range of social services for its residents. Solutions proposed by the American Heart Association and American Stroke Association, such as expanding Medicaid, investing in the rural workforce, and promoting economic development in rural areas, are also important steps to reducing risk for cardiovascular disease.
Data and Methods
Data. For the study, the authors merged 16 years of geocoded birth certificate data in Texas with neighborhood- and county-level data. The birth certificate data covered births between 2005 and 2020 to mothers aged 30 to 45 years, and the final sample size was 2,089,588 births. Neighborhood-level, or Census tract-level data, came from the American Community
Survey. County-level data for Texas came from the National Center for Health Statistics Urban-Rural Classification Scheme for Counties.
Variables. Dependent, or outcome, variables included pre-pregnancy diabetes, hypertension, obesity, and smoking. Independent, or predictor, variables included individual-level race and ethnicity, country of birth, educational attainment, the percentage of poor people within neighborhoods, racial and ethnic concentrations within neighborhoods, and urban or rural status of counties. The authors controlled for other sociodemographic characteristics (age, marital status) and time trends.
Analysis. The authors first calculated percentages of the four risk factors to describe the prevalence of each risk factor for all individual-, neighborhood-, and county-level variables. Then, they used two-level, random intercept hierarchical generalized logistic models to estimate associations and model fit.
Reference
[1] Cubbin, C., La Frinere-Sandoval, Q.N.B., & Widen, E.M. (2025). Social inequities in cardiovascular disease risk factors at multiple levels persist among mothers in Texas. International Journal of Environmental Research and Public Health, 22(404). https://doi.org/10.3390/ijerph22030404
Suggested Citation
Cubbin, C., La Frinere-Sandoval, Q.N.B., & Widen, E.M. (2025). Inequities among individuals, neighborhoods, and counties affect the likelihood of cardiovascular disease for mothers during the “rush hour of life.” Population Research Center Research Brief 10(6). https://doi.org/10.26153/tsw/60952.
About the Authors
Catherine Cubbin, ccubbin@austin.utexas.edu, is the Clara Pope Willoughby Centennial Professor in Community Safety in the School of Social Work and a faculty scholar at the Population Research Center at The University of Texas at Austin; Quynh Nhu (Natasha) B. La Frinere-Sandoval is a PhD student in the School of Social Work at UT Austin; Elizabeth M. Widen is associate professor in the Department of Nutritional Sciences, College of Natural Sciences and a faculty scholar at the Population Research Center, UT Austin.
Acknowledgements: This work was supported by a grant from the Texas Center for Equity Promotion at the University of Texas at Austin and grant P2CHD042849 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) awarded to the Population Research Center at UT Austin. Other support derived from grant T32HL140290 from the National Heart, Lung, and Blood Institute (PI: Cubbin), grants (R01ES034803, R01ES035131) from the National Institute of Environmental Health Sciences (PI: Cubbin), grant NUR3DD000114 from the Centers of Disease Control and Prevention (PI: Cubbin), and grant R00HD086304 from the NICHD (PI: Widen). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or other funders.